Part 1 of 2
Vaginal Douching: Evidence for Risks or Benefits to Women's Healthby Jenny L. Martino and Sten H. Vermund
Epidemiol Rev. 2002; 24(2): 109–124.
INTRODUCTIONVaginal douching is the process of intravaginal cleansing with a liquid solution. Douching is used for personal hygiene or aesthetic reasons, for preventing or treating an infection(1), to cleanse after menstruation or sex, and to prevent pregnancy (2). For at least 100 years, there have been conflicting views on the benefits or harm in douching. Although there is a broad consensus that douching should be avoided during pregnancy, there is less agreement regarding douching for hygiene and relief of vaginitis symptoms. Two earlier reviews of douching data in women (3) and adolescents (4) have concluded that douching is harmful and should be discouraged because of its association with pelvic inflammatory disease, ectopic pregnancy, and perhaps other conditions. Nonetheless, douching continues to be a common practice.
We seek to review the evidence of the impact of douching on women's health.METHODSStudies included in this review were identified via a search of the computerized MEDLINE database from 1965 through March 2002. Only English-language articles were included, as were a few relevant articles published before 1965. Major medical and nursing organizations were contacted for their policy and educational documents. Via a Freedom of Information request, we secured a summary of the Nonprescription Drug Advisory Committee meeting held on April 15, 1997, from the US Food and Drug Administration.
EPIDEMIOLOGY OF DOUCHINGDouching products (table 1), methods, frequency, motivation, and timing can vary considerably among women who douche.
The prevalence of douching has decreased since 1988, but it is still a common practice among American women, especially adolescents, African-American women, and Hispanic women (table 2) (1, 5). In 1995, 55 percent of non-Hispanic Black women, 33 percent of Hispanic women, and 21 percent of non-Hispanic White women reported “regular” douching (5). In the United States, there have been reports of 52-69 percent of adolescents douching at least once and one study documenting 56 percent reporting douching one or more times a week (2, 6-8).
In addition, douching is prevalent in some African countries, such as Côte d'Ivoire, where the douching rate among women has been reported to exceed 97 percent (9). It is uncommon for women to douche daily; sporadic douching is more common (1, 8). A dose-response relation between douching and its adverse effects has been found by some, highlighting the importance of assessing douching frequency in any related research (10-14).
The intensity and method of douching, especially douching with pressure, have been associated with adverse outcomes (15).
TABLE 1
Some vaginal douching products*
Ingredients / Function / Commercial / Home preparation
5% acetic acid (vinegar) / Acidifying agent / X / X
Benzoic acid, citric acid, lactic acid, sorbic acid / Acidifying agents / X / --
Bleach (sodium hypochlorite and sodium hydroxide) / Cleanser / X/ --
Cetylpyridinium chloride / Antimicrobial, antiseptic, germicidal, surfactant / X / --
Decyl glucoside / Nonionic detergent, mild surfactant, solubilizes water-insoluble materials / X / --
Diazolidinyl urea / Acidifying agent / X / --
Disodium EDTA,† edetate† disodium / Preservative, antibacterial agent, metal chelator (binds magnesium and calcium) / X / --
Lysol (alkyl 50% C14, 40% C12, 10% C16, dimethylbenzyl-ammonium chloride 2.7%; Reckitt & Coleman, Wayne, NJ) / Cleanser / -- / X
Octoxynol-9 / Surfactant, produces a mucolytic or proteolytic effect, spermicide / X / --
Povidone-iodine‡ / Antimicrobial / X / --
SD Alcohol 40† / Liquid vehicle / X / --
Sodium benzoate / Preservative (prevents bacteria from growing in solution that contains citrate and lactate) / X / --
Sodium bicarbonate (baking soda) / Alkalizing agent / X / X
Sodium citrate / Acidifying agent / X / --
Sodium lactate / Acidifying agent / X / --
Water / Liquid vehicle, cleansing / X / X
Yogurt / Potential source of nonhuman strain of lactobacillus / -- / X
*Sources: Handbook of Nonprescription Drugs. Washington, DC: American Pharmaceutical Association and the National Professional Society of Pharmacists, 1982; and Dr. Dennis Pillion, Pharmacology Department, University of Alabama at Birmingham, personal communication, 2001.
†EDTA, ethylenediaminetetraacetic acid; edetate, ethylenediaminetetraacetate; SD Alcohol 40, specially denatured alcohol, followed by a number or a number-letter combination that indicates how the alcohol was denatured, according to the formulary of the US Bureau of Alcohol, Tobacco, and Firearms.
‡Medicated douches.
TABLE 2
Percentage of women who douche regularly, by age and race/ethnicity, according to the National Survey of Family Growth, United States
Year and reference / Sample size(no.) / Age (years) / Total (%) / Non-Hispanic Black (%) / Non-Hispanic White (%) / Hispanic (%)
NSFG,*1995(5) / 10,847 / 15-44 / 26.9 / 55.3 / 20.8 / 33.4
NSFG,*1995(5) / 10,847 / 15-19 / 15.5 / 36.8 / 10.8 / 16.4
NSFG,*1995(5) / 10,847 / 20-24 / 27.8 / 60.4 / 20.4 / 32.5
NSFG,*1995(5) / 10,847 / 25-29 / 30.0 / 58.7 / 23.9 / 38.0
NSFG,*1995(5) / 10,847 / 30-34 / 30.6 / 60.4 / 24.5 / 35.1
NSFG,*1995(5) / 10,847 / 35-39 / 28.9 / 62.5 / 21.9 / 41.2
NSFG,*1995(5) / 10,847 / 40-44 / 26.9 / 53.1 / 21.1 / 38.5
Year and reference / Sample size(no.) / Age (years) / All races (%) / Black (%) / White (%)
NSFG, 1988(1) / 8,450 / 15-44 / 36.7 / 66.5 / 32.0
NSFG, 1988(1) / 8,450 / 15-19 / 31.0 / 53.5 / 25.4
NSFG, 1988(1) / 8,450 / 20-24 / 41.1 / 63.1 / 35.7
NSFG, 1988(1) / 8,450 / 25-29 / 37.6 /67.6 / 32.9
NSFG, 1988(1) / 8,450 / 30-34 / 36.0 / 64.8 / 31.5
NSFG, 1988(1) / 8,450 / 35-39 / 35.1 / 70.2 / 30.2
NSFG, 1988(1) / 8,450 / 40-44 / 37.0 / 65.8 / 33.8
*NSFG, National Survey of Family Growth.
The timing of douching may impact on adverse sequelae, such as the temporal use of douching in relation to sexual activity, pregnancy, symptoms, and the menstrual cycle (4, 11, 16, 17). During ovulation, the levels of circulating estrogens increase, the cervical os opens, and the cervical mucus becomes clearer and more profuse (3, 18). Therefore, the risk of ascending infection from the pressure of douching may be greatest around the time of ovulation when the cervical os is gaping and the mucus is thin (3).Women who douche consider it to be a healthy practice and often state that hygiene is their primary reason for douching (2, 6, 8, 15, 19). Some women state that douching is “necessary for good hygiene” (19). Motives for douching are many: to cleanse the vagina after menses or before or after sexual intercourse, to prevent or ameliorate an odor, to prevent or treat vaginal symptoms such as itching and discharge, and, less commonly, to prevent pregnancy or sexually transmitted diseases (2).
Most women report douching for hygienic reasons, while douching due to symptoms may be comparatively uncommon (20, 21).
Outside influences such as physicians, mothers, girlfriends, boyfriends, and the media affect a woman's decision to douche (19). The motivation for douching is a complicated issue imbued with both psychologic and social features that need to be addressed if vaginal douching behavior is likely to be modified on any large scale.
HEALTH EFFECTS OF DOUCHINGDouching has been associated with many adverse outcomes including pelvic inflammatory disease, bacterial vaginosis, cervical cancer, low birth weight, preterm birth, human immunodeficiency virus transmission, sexually transmitted diseases, ectopic pregnancy, recurrent vulvovaginal candidiasis, and infertility. Studies conflict, however, and the strength of association varies enormously between studies. Many potentially confounding factors blur the epidemiologic assessment of the consequences of douching. Douching in the United States is more common among African-American women (1, 3, 5, 19). Independently of race, associations between douching and poverty, less than a high school education, a history of pelvic inflammatory disease, and having between two and nine lifetime sexual partners are reported (1). A lower educational level, many sexual partners, and poverty are also risk factors for sexually transmitted diseases and bacterial vaginosis, making it especially complicated to assess causality since women might douche secondary to infection-related symptoms rather than for routine purposes.
Conflicting results are reported regarding sexually transmitted infections and douching. Some studies suggest that adolescents who douche are more likely to have a history of a sexually transmitted disease (1, 15), while other studies have found that women who have a history of a sexually transmitted disease were less likely to douche (1, 10, 22). Prospective studies are needed to assess whether douching is causally related to sexually transmitted diseases or if douching is most commonly a response to symptomatic vaginitis. Whether complications like pelvic inflammatory disease might have occurred even without douching can be answered with prospective studies (1, 23, 24).
PHYSIOLOGYThere are several ways by which douching may contribute to disease. Douching may remove normal vaginal flora, permitting the overgrowth of pathogens. It may also provide a pressurized fluid vehicle for pathogen transport, helping lower genital tract infections ascend above the cervix into the uterus, fallopian tubes, or abdominal cavity (3, 16). These microbiologic and physical mechanisms may work in concert. Ness et al. (25) found that, among a group of women with clinical pelvic inflammatory disease, frequent and recent douching was associated with endometritis and upper genital tract infection in women with normal or intermediate vaginal flora, although this was not noted in women with bacterial vaginosis.
An added concern is that, if douching reduces the density of normal vaginal flora, bacterial vaginosis might develop or there may be a predisposition to colonization by such sexually transmitted pathogens as Neisseria gonorrhoeae or Chlamydia trachomatis, filling the “ecologic niche” (16). Pathogenic bacteria may then ascend into the upper reproductive tract, leading to inflammatory scarring (endometritis, salpingitis, or peritonitis), the principal cause of ectopic pregnancy, early miscarriage, and infertility (16).
Physiologic risk for sexually transmitted diseases is greater among adolescent women, since they typically have ectopic columnar epithelial cells in the exocervix with a large transformation zone that is vulnerable to bacterial and viral sexually transmitted infections (26). Some argue that it is especially important to caution adolescents about the potential adverse effects of douching, as they may be even more susceptible to its adverse consequences (4).DOUCHING AND VAGINAL ECOLOGYA healthy menarcheal vaginal environment is composed primarily of lactobacilli (27). Hydrogen peroxide (H2O2)-producing lactobacilli may protect the vagina against the overgrowth of potentially pathogenic indigenous flora and exogenous pathogens. Selected human strains of lactobacilli produce lactic acid that helps keep the vaginal pH low, usually less than 4.5, which is inhospitable to many pathogenic organisms (28). In addition to H2O2 production, lactobacilli adhere to epithelial cells, block pathogen adhesion, and stimulate the mucosal immune system (28).
Newton et al. (29) found that douching more than once per month was associated with the presence of Trichomonas vaginalis (odds ratio (OR) = 3.5, p = 0.02) and that douching one or more times a month was associated with Gardnerella vaginalis (OR = 2.4, p = 0.05). They examined Mexican-American and African-American women and concluded that race (specifically, being African American) had a more consistent association with the presence or absence of a cervical-vaginal organism than other factors, including behavioral variables.
Different types of douching liquids have various antimicrobial effects.
Pavlova and Tao (30) used in vitro studies to show that four antiseptic douches were inhibitory against all vaginal microorganisms, including lactobacilli. Three vinegar-containing douches selectively inhibited vaginal pathogens associated with bacterial vaginosis, group B streptococcal vaginitis, and candidiasis, but not lactobacilli, suggesting to the investigators that vinegar (5 percent acetic acid) douches may be less harmful or may be beneficial. Juliano et al. (31) tested seven commercial vaginal antiseptic douche solutions against vaginal lactobacilli and found marked in vitro antibacterial activity, often after very short exposure times. Thus, some douche preparations may cause substantial changes in vaginal flora.
Onderdonk et al. (32) found that healthy women who douched with a 4 percent acetic acid solution experienced a transient reduction of total bacteria that they attributed to the physical washing of the vaginal vault alone. However, when they used povidone-iodine, a bactericidal agent, it caused a significant reduction in total bacterial counts that suggested an antiseptic effect in addition to the washing effect.
They concluded that, in some individuals, douching may decrease the vaginal bacteria that are present, allowing a rapid proliferation of potential pathogens, increasing the risk of associated infections. In contrast, Monif et al. (33) found that, while in vivo douching with povidone-iodine caused a dramatic decrease in the total number of vaginal bacteria, baseline counts were reestablished within 120 minutes. They also found that lactobacilli were the first bacteria to recover. As a consequence,
Monif (34) has argued for the potential benefits of douching. However, these experiments do not reflect that some women may participate in a behavior that alters the vaginal ecology before it has a chance to return to normal, such as repeated douching or vaginal or receptive vaginal, oral, or anal sex]. The weight of the epidemiologic evidence suggests that repeated douching with its attendant washing and antibacterial effects will diminish lactobacilli predominance and risk reproductive tract infections.BACTERIAL VAGINOSISBacterial vaginosis is a common cause of malodorous vaginal discharge in women (35). Three million symptomatic cases are reported annually in the United States, but millions more remain unreported or unrecognized (28, 36). A clinical diagnosis of bacterial vaginosis requires three of the following “Amsel criteria”: vaginal pH of greater than 4.5, a positive “whiff” test for amines, presence of clue cells, and a thin homogenous discharge (37).
In women with bacterial vaginosis, lactobacilli, especially H2O2-producing lactobacilli, are greatly decreased and the vagina becomes overgrown with anaerobic and facultatively anaerobic bacteria that are often present in small numbers in the normal vagina. These include G. vaginalis, Mycoplasma hominis, Prevotella spp., Peptostreptococcus spp., Mobiluncus spp., and Bacteroides spp. (28, 38-40).
Bacterial vaginosis has been reported to be twice as common among African-American and Afro-Caribbean women than among White women (35, 41-44). Vaginal douching is also twice as common among African-American women. It has been proposed that bacterial vaginosis is sometimes sexually transmitted; however, no male factor has been identified, and bacterial vaginosis can occur in adolescent women who have never had sexual intercourse (45).
Bacterial vaginosis is common, and many factors reminiscent of sexually transmitted disease risk are associated with bacterial vaginosis. Schwebke et al. (46) found that 78 percent of women without evidence of genital tract infection had significant, although transient, changes in their vaginal flora. Day-to-day variability was defined as less than 85 percent of a given woman's normal vaginal flora, which was calculated on data from self-obtained vaginal smears from each woman. In a multivariable analysis, more frequent episodes of receptive oral sex were associated with unstable flora. Day-to-day variability in vaginal flora was associated with the use of vaginal medication, menses, greater number of sexual partners, spermicide use, more frequent vaginal intercourse, and less frequent use of condoms. Many of these factors are also associated epidemiologically with bacterial vaginosis and sexually transmitted diseases.
It has also been reported that intrauterine device users are more likely to be diagnosed with bacterial vaginosis than are nonusers (47).
Bacterial vaginosis has been linked with several adverse reproductive outcomes, including endometritis (48-51), spontaneous preterm delivery (52-61), preterm delivery of low birth weight infants (62), low birth weight (13), premature rupture of the membranes (52, 55), histologic chorioamnionitis (63), and infection of amniotic fluid (64-66). In a randomized clinical trial, Hauth et al. (67) studied pregnant women with bacterial vaginosis who also had a high risk for preterm delivery. Antepartum metronidazole and erythromycin lowered the frequency of prematurity. However, two other studies found that vaginal clindamycin for treatment of bacterial vaginosis did not decrease the rate of preterm deliveries (68, 69). The frequency of vaginal douching was shown by Fiscella et al. (13) to have a dose-response relation with the likelihood of low birth weight.
If a pregnant woman has bacterial vaginosis and douches, chronic bacterial colonization of the endometrium and/or chorioamnion may cause preterm rupture of the membranes and/or preterm labor (70). Meis et al. (60) found that the presence of bacterial vaginosis at 28 weeks' gestation is associated with an increased risk of spontaneous preterm birth, defined as birth at less than 35 weeks. This association is strongest for early preterm birth and may be mediated by subclinical chorioamnionitis (71).
Douching is associated with bacterial vaginosis, although the direction of causation is uncertain: Does douching predispose to bacterial vaginosis, or do women douche in response to bacterial vaginosis symptoms? In a cross-sectional study, Holzman et al. (72) found that vaginal douching within the past 2 months was associated with an increased prevalence of bacterial vaginosis (OR = 2.9, 95 percent confidence interval (CI): 1.5, 5.6).
Fonck et al. (73) found that, in female sex workers in Nairobi, Kenya, douching in general and douching with soap and water were both significantly associated with bacterial vaginosis, with a significant trend for increased frequency of douching and higher prevalence of bacterial vaginosis. In an important recent prospective cohort study, Royce et al. (74) found that douching was associated with bacterial vaginosis (risk ratio (RR) = 1.8, 95 percent CI: 1.7, 2.0) and preterm birth (RR =1.6, 95 percent CI: 1.1, 2.1). Rajamanoharan et al. (35) found that bacterial vaginosis was strongly associated with the use of commercial antiseptic products applied to the vulval mucosa or as a vaginal douche. After controlling for genital hygiene behaviors (such as douching and vulval antiseptics) and history of previous bacterial vaginosis episodes, they found that there were no ethnic differences between women with bacterial vaginosis and women without bacterial vaginosis. Hawes et al. (44) found that lack of vaginal H2O2-producing lactobacilli was independently associated with bacterial vaginosis but not with vulvovaginal candidiasis. They also reported that acquisition of bacterial vaginosis was associated with having a new sexual partner and douching for hygiene. Stevens-Simon et al. (75) found that Black adolescents had a more alkaline vaginal pH than did White adolescents, possibly decreasing their resistance to common vaginal infections, such as trichomoniasis and bacterial vaginosis.
Given the frequency of bacterial vaginosis among American women and its associations with adverse reproductive outcomes, the largest attributable risk for which douching may be responsible may be increased bacterial vaginosis frequency. However, the temporal relation has not been well established given the paucity of large, prospective studies.
GONORRHEA, CHLAMYDIA, AND OTHER SEXUALLY TRANSMITTED DISEASESMany sexually transmitted diseases are asymptomatic and therefore go undiagnosed, particularly in women. Two bacterial sexually transmitted diseases, gonorrhea and chlamydia, are especially important causes of pelvic inflammatory disease. Chlamydia has been associated with tubal infertility due to fallopian tube scarring and obstruction (76-80), ectopic pregnancy (81), and pelvic inflammatory disease (82). In addition, both
chlamydia and gonorrhea have been reported to facilitate human immunodeficiency virus transmission (26). Several studies have found an association between douching and chlamydial infection (9, 14, 25, 83-85). However, cross-sectional studies cannot determine reliably whether the douching preceded the disease or if the symptoms led to the douching.
Scholes et al. (14) found that women who reported douching 12 months prior to their clinic visit were twice as likely to have cervical chlamydial infection and that, as the frequency of douching increased, the likelihood of chlamydial infection also increased. Peters et al. (83) found that douching at least monthly was significantly associated with chlamydia in adolescents. Beck-Sague et al. (84) found that, in adolescents who douched monthly or more frequently, there was a higher prevalence of chlamydia.
Stergachis et al. (85) found that douching within the last year was independently predictive of chlamydial infection.
Other studies have examined sexually transmitted diseases in general. Foch et al. (7) found that, in adolescents attending a family planning clinic,
those who reported douching were more likely to have a history of a sexually transmitted disease. Joesoef et al. (17) found that, among Indonesian pregnant women, douching with water and soap, betel leaf, or a commercial agent after sex was associated with having a sexually transmitted disease and that the association was strengthened among women who douched before sex or both before and after sex. Compared with women who never douched, those who always douched with betel leaf or a commercial agent had a substantially increased risk for sexually transmitted diseases (OR = 9.4, 95 percent CI: 1.8, 50.3). Douching with irritating substances may make the vaginal mucosa more susceptible to sexually transmitted diseases, analogous to the use of intravaginal herbs as drying agents (86). Critchlow et al. found that cervical ectopy, which has been associated with acquisition of certain sexually transmitted diseases, including chlamydia (87, 88) and human immunodeficiency virus (89), was less common among women with sexually transmitted diseases who douched recently (90). Douching and sexual activity both may accelerate squamous metaplasia and cervical maturation (91, 92). Cervical ectopy is common in adolescents and has been associated with increased risk of sexually transmitted disease acquisition, suggesting the importance of measuring all these factors together in studies of douching and health risk (87, 88, 91). Jacobson et al. (91) found that both douching and sexual activity may decrease ectopy in adolescents. If women who douche have less ectopy, they might eventually have a theoretically lower chance to acquire sexually transmitted diseases, although there are no data that suggest this. In contrast to the above studies, Fonck et al. (73) found that, in female sex workers in Nairobi, Kenya, there was no direct relation between douching and the risk for human immunodeficiency virus infection or other sexually transmitted infections. Similarly, Moscicki et al. (92) found no ectopy association with human immunodeficiency virus among US adolescents.
Given the severity of the reproductive consequences of gonorrhea and chlamydia, the associations with douching are worrisome, particularly for chlamydia. As with bacterial vaginosis, the temporal relation is clouded by the paucity of prospective data, hindering clarification of whether douching is a cause or a consequence.
PELVIC INFLAMMATORY DISEASEPelvic inflammatory disease is a polymicrobial infection primarily initiated by ascending infection to the upper reproductive tract by N. gonorrhoeae, C. trachomatis, or anaerobic and/or facultative bacteria also occurring with bacterial vaginosis (93-96). It is virtually certain that the physical pressure of douching can facilitate ascension of pathogens (23). Infection, inflammation, and scarring of the fallopian tubes, ovaries, and/or the uterine lining can result in tubal infertility, tuboovarian abscess, endometritis, chronic pelvic pain, recurrent pelvic inflammatory disease, and ectopic pregnancy. Pelvic inflammatory disease affects over 1 million American women and adolescents annually at an estimated cost of $4.2 billion in 1990 (94, 97).
The total cost of pelvic inflammatory disease, including both direct and indirect costs, was projected to be more than $9 billion in 2000 (97). It was estimated that 20-30 percent of women with pelvic inflammatory disease would be hospitalized (24) and that at least 25 percent would suffer one or more serious long-term sequelae (97). Guidelines for diagnosis from the Centers for Disease Control and Prevention include complaint of abdominal pain and clinical findings of lower abdominal, cervical motion, and adnexal tenderness (98). Silent pelvic inflammatory disease that goes unreported may account for 50 percent or more of all the cases of pelvic inflammatory disease (99).
About 70 percent of the women diagnosed with pelvic inflammatory disease in the United States are under 25 years of age (100). Risk factors for pelvic inflammatory disease have been found to include being of lower socioeconomic status, non-White, less than 25 years of age, being exposed to a sexually transmitted disease or having a history of pelvic inflammatory disease, use of an intrauterine device, failure to use contraception, multiple sexual partners, and earlier sexual initiation (100, 101). Some of these same characteristics are prevalent among women who douche, and vaginal douching has been associated with pelvic inflammatory disease in most studies (3, 12, 22, 26, 102-107).
Vaginal douching may potentially increase the risk of pelvic inflammatory disease by promoting the ascension of lower genital tract infections to the upper genital tract, by changing the vaginal environment to increase susceptibility to reproductive tract infections that precede pelvic inflammatory disease, or by introducing nonpathogenic vaginal bacteria into the typically sterile upper genital tract (24). The weight of the evidence suggests a causal association of douching and pelvic inflammatory disease, but the lack of prospective studies continues to plague efforts to clarify the causal relation.
As early as 1952, an association between douching and pelvic inflammatory disease was suspected (108). Jossens et al. (106) found that douching after menses was a significant risk factor for pelvic inflammatory disease. Others report uncertainty (109) in the relation between douching and pelvic inflammatory disease or have found vaginal douching to be associated with pelvic inflammatory disease (107, 110) (figure 1) (3, 10, 95, 104, 106, 110, 111). Mueller et al. (111) found that women who douched had moderately elevated risks for overt and silent pelvic inflammatory disease-associated infertility. Scholes et al. (104) found that women who douched during the previous 3 months had an elevated odds ratio for pelvic inflammatory disease of 2.1 after controlling for other risk factors.
They also found that there was a dose-response relation as women who douched more frequently had a higher pelvic inflammatory disease risk. In a case-control study, Wolner-Hanssen et al. (10) found that current douching was more common among women with pelvic inflammatory disease and that pelvic inflammatory disease was significantly related to frequency of douching. Neumann and DeCherney (102) found an association between pelvic inflammatory disease and vigorous and frequent (more than once a week) douching. Miller et al. (26) reported douching to have a significant impact on the risk of pelvic inflammatory disease. Forrest et al. (22) reviewed the literature through 1989 and concluded that the weight of published evidence supported an association between vaginal douching and both pelvic inflammatory disease and ectopic pregnancy. Zhang et al. (3) reported in a 1997 meta-analysis that douching increased the risk of pelvic inflammatory disease by 73 percent. Miller et al. (26) found that, from the 1995 National Survey of Family Growth, douching was significantly associated with having pelvic inflammatory disease. Aral et al. (103) analyzed data from the 1988 National Survey of Family Growth and found that almost 11 percent of American women had a history of treatment for pelvic inflammatory disease. They suggested that vaginal douching increased the risk of pelvic inflammatory disease by 50 percent among White and by 30 percent among African-American women.
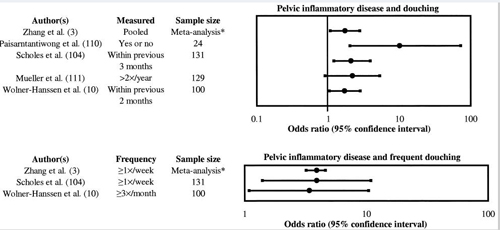
FIGURE 1
Pelvic inflammatory disease and douching. Top: This figure represents the odds ratio and 95% confidence interval from several studies that looked at pelvic inflammatory disease and douching. Bottom: This figure represents the odds ratio and 95% confidence interval from several studies that looked at pelvic inflammatory disease and various frequencies of douching. *, estimated n = 231 based on two studies (10, 104).
Pelvic inflammatory disease is a prevalent problem worldwide as well as in the United States. Its serious reproductive outcomes and financial burdens are a major factor motivating sexually transmitted disease control and prevention. The weight of the evidence suggests strongly an association between pelvic inflammatory disease and douching. This association may represent the strongest incentive for policies to discourage women from douching.REDUCED FERTILITY, INFERTILITY, AND ECTOPIC PREGNANCYPelvic inflammatory disease is a common cause of reduced fecundity (fertility) and sterility (112, 113). In an analysis of the 1995 National Survey of Family Growth, it was found that women with a history of pelvic inflammatory disease were less likely to be fecund compared with women with no such history (26). The likelihood of infertility increases as the number and severity of pelvic inflammatory disease episodes increase (26).
It has been reported that 20 percent of women who have one episode of pelvic inflammatory disease will be infertile (114) and that 50 percent of women who have three or more episodes of pelvic inflammatory disease will be infertile (115). Vaginal douching may reduce fecundity by increasing susceptibility to infection (11). Baird et al. (11) found that women who douched were 30 percent less likely to become pregnant each month compared with women who did not douche. This risk was greater for younger women than it was for older women.Ectopic pregnancy is defined as implantation of a fertilized egg outside the uterine cavity (116). Women with a history of pelvic inflammatory disease were twice as likely to have had an ectopic pregnancy compared with sexually active women who had no history of pelvic inflammatory disease (26). Vaginal douching has been associated with ectopic pregnancy (117-119).
Several studies reported that vaginal douching increased the risk for ectopic pregnancy (figure 2) (3, 84, 120-123). Daling et al. (121) found that there was a small increase in risk of tubal pregnancy among women who douched more than two times per year in the past year (RR = 1.3, 95 percent CI: 0.9, 1.8). This risk was found to increase further if, in addition to douching more than two times per year, the women also had more than one sexual partner during their lifetime (RR = 1.6, 95 percent CI: 1.1, 2.3) or had previous exposure to chlamydia (RR = 2.4, 95 percent CI: 0.8, 7.3).
Kendrick et al. (123) found that ectopic pregnancy risk among African-American women correlated with the number of years of douching at least once per month. They found that any douching carried some risk and that different douching strategies were associated with different levels of risk. In a case-control study that controlled for chlamydial exposure, J. M. Chow et al. (81) found that current douching was an independent risk factor for ectopic pregnancy. In a different study, W. H. Chow et al. (120) reported that the risk of tubal ectopic pregnancy for women who douched at least weekly was twice that of women who never douched. In a meta-analysis, Zhang et al. (3) found that frequent douching increased risk of ectopic pregnancy by 76 percent. In a meta-analysis of case-control and cohort studies done between 1978 and 1994, Ankum et al. (118) found only a slightly increased risk for ectopic pregnancy due to douching. However, in a case-control study of ectopic pregnancy with 69 cases and 101 controls, Phillips et al. (122) found that there was not a significant increase in the risk of ectopic pregnancy due to vaginal douching once or more per month (OR = 0.8, 95 percent CI: 0.3, 2.2).
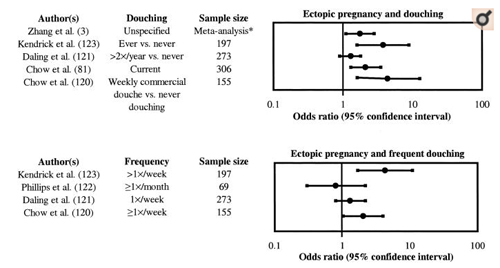
FIGURE 2
Ectopic pregnancy and douching. Top: This figure represents the odds ratio and 95% confidence interval from several studies that looked at ectopic pregnancy and douching. Bottom: This figure represents the odds ratio and 95% confidence interval from several studies that looked at ectopic pregnancy and various frequencies of douching. *, estimated n = 1,000 based on five studies (81, 120-123).
Bacterial infections of the lower and upper genital tracts can result in pelvic inflammatory disease, which can, in turn, result in reduced fertility, infertility, and ectopic pregnancy. Many studies have looked at ectopic pregnancy risk and douching, with the majority of evidence finding an association. The temporal relation here remains problematic with the dearth of prospective studies.
CERVICAL CANCERCervical cancer is among the most common cancers in women worldwide (124). The American Cancer Society estimates that, during 2001, about 12,900 cases of invasive cervical cancer would be diagnosed in the United States and that about 4,400 American women would die from cervical cancer (125). Cervical cancer was once one of the most common causes of cancer death for American women but now, due to early detection and treatment, it is far less so (125). Worldwide, cervical cancer is the second or third most common cancer among women and, in some developing countries, it is the most common women's cancer (126).
Nearly all squamous cell cervical cancer cases are related to human papillomavirus, a sexually transmitted infection. The cause of cervical cancer has been postulated to be multifactorial, with other cofactors being required to cause cancer.
Haverkos et al. (127) proposed that tar exposure through tar-based vaginal douching products may be one such cofactor, increasing the risk of invasive cervical cancer. Cervical cancer is twice as high among African-American women as among White women, as are douching rates.A positive relation between the frequency of douching and cervical cancer risk was found in several studies (figure 3)(3, 128-134).
Graham and Schotz (128) found that, as the frequency of douching increased, so did the risk of invasive cervical cancer and carcinoma in situ. Peters et al. (129) found that the “frequency-years” of douching contributed independently and significantly to the risk of invasive cervical cancer. In a meta-analysis, Zhang et al. (3) found that douching was modestly associated with cervical cancer, when they aggregated studies that looked at both invasive cervical cancer and carcinoma in situ together or at invasive cervical cancer alone (RR = 1.25, 95 percent CI: 0.99, 1.59). However, it is unclear whether this risk ratio refers to invasive cervical cancer or both carcinoma in situ and invasive cervical cancer combined. Zhang et al. reported that, among women who douched at least once a week, the pooled adjusted risk ratio was 1.86 (95 percent CI: 1.29, 2.68). In a population-based case-control study in Utah, Gardner et al. (132) looked at a combined study group of invasive cervical cancer (13 percent of the study group) and carcinoma in situ (87 percent of the study group) and found no association between cervical cancer and douching in women who douched once per week or less. However, in women who douched more than once a week, a positive association was found (OR = 4.7, 95 percent CI: 1.9, 11). They hypothesized that
douching alters the vaginal chemical environment, making the cervix more susceptible to pathologic changes and subsequent cervical cancer.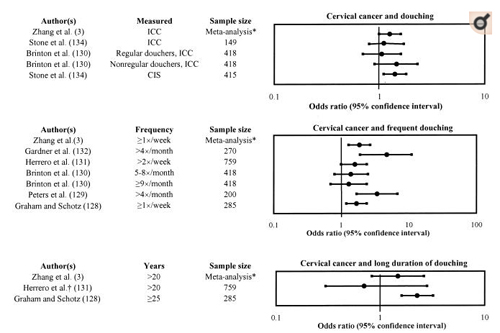
FIGURE 3
Cervical cancer and douching. Top: This figure represents the odds ratio and 95% confidence interval from several studies that looked at cervical cancer and douching. Middle: This figure represents the odds ratio and 95% confidence interval from several studies that looked at cervical cancer and various frequencies of douching. Bottom: This figure represents the odds ratio and 95% confidence interval from several studies that looked at cervical cancer and long durations of douching. CIS, carcinoma in situ; ICC, invasive cervical cancer. *, estimated n = 2,081 based on six studies (128-132, 134); †, error in original paper as to lower bound of 95% confidence interval: 0.8; our estimate of likely correct lower bound: 0.3.
In contrast, in a population-based case-control study in Costa Rica, Stone et al. (134) found that douching was not associated with carcinoma in situ or invasive cervical cancer. Herrero et al. (131), in a case-control study in Latin America, found no consistent association between vaginal douching and invasive cervical cancer. In a case-control study, Brinton et al. (130) found inconsistent results related to the risk of vaginal douching and invasive cervical cancer. They found 30-40 percent nonsignificant elevations in invasive cervical cancer risk associated with regular douching of five or more times per month, but they also found that nonregular douchers were at a higher risk than were regular douchers and that there was no clear relation to the age of first douching or total months of use. They therefore hypothesized that the association they observed may just represent chance.
Cervical cancer is a common cancer in women. Studies on cervical cancer and douching do not show a clear association, with some studies showing a positive association, some a negative association, and some no association. Although cervical cancer would not generate symptoms that might motivate a woman to douche, it is more common among women with other sexually transmitted disease risk factors. For a definitive assessment of causality, a prospective determination would be needed, a difficult task for a chronic disease with a long latency period.
HUMAN IMMUNODEFICIENCY VIRUSSexually transmitted diseases and other genital tract infections have been implicated in the acquisition and transmission of human immunodeficiency virus (135-137).
Vaginal flora abnormalities, including bacterial vaginosis and sexually transmitted diseases, have been found to be associated with human immunodeficiency virus infection (138-140).
Normal vaginal acidity can partly inactivate human immunodeficiency virus, so if bacterial vaginosis raises the pH of vaginal fluid and recruits target inflammatory cells, women with bacterial vaginosis may be more susceptible to human immunodeficiency virus. H2O2-producing lactobacilli have been shown to have viricidal effects on human immunodeficiency virus type 1 (141), and a low vaginal pH may reduce the number of human immunodeficiency virus type 1 target cells in the vagina (142).
Helfgott et al. (143) found significant associations between human immunodeficiency virus and bacterial vaginosis, vulvovaginal candidiasis, and trichomonal vaginitis. In a study in Côte d'Ivoire, human immunodeficiency virus was found to be two times more frequent in women using intravaginal antiseptics (9). These cross-sectional studies could be confounded in that bacterial vaginosis, sexually transmitted diseases, and human immunodeficiency virus can be consequences of high risk sexual behavior, although several studies used logistic regression modeling to try to control for sexual behavior.
Not all douching products would be expected to carry comparable risks. Gresenguet et al. (86), in Bangui, Central African Republic, found that vaginal douching with noncommercial preparations was associated with an increased prevalence of human immunodeficiency virus, whereas douching with commercial antiseptic preparations was associated with a lower prevalence of this virus. However, the median years of education for women using commercial antiseptics was 8 years, compared with only 2 years for women using noncommercial preparations, so the results may be confounded by socioeconomic status. Tevi-Benissan et al. (144) reported that vaginal douching reduces semen load substantially after sexual intercourse, and they suggested douching as a supplementary means for prevention of heterosexual human immunodeficiency virus transmission. Given the associations of douching with bacterial vaginosis/sexually transmitted diseases, such a policy suggestion should be studied carefully as other data suggest douching to be harmful.
The relation among human immunodeficiency virus, bacterial vaginosis, and sexually transmitted diseases is complex, as all may be contributed to by high risk sexual behavior. Only a few cross-sectional studies have looked at human immunodeficiency virus and douching, suggesting concern that douching might be associated with risk for human immunodeficiency virus. Given the vast pool of women infected worldwide with human immunodeficiency virus, other sexually transmitted diseases, and bacterial vaginosis and the increased risk attributable to douching, education to discourage douching by women may have a huge impact on the risks of infections and reproductive health consequences.