Re: Mindfulness Meditation Research: Issues of Participant S
Adverse Effects of Meditation: A Preliminary Investigation of Long-Term Meditators
by Deane H. Shapiro, Jr., Ph.D.
International Journal of Psychosomatics, Vol. 39 (Nos. 1-4), 1992 63
Manuscript submitted June 30, 1991 and accepted May 1 1992.
NOTICE: THIS WORK MAY BE PROTECTED BY COPYRIGHT
Adverse effects of meditation were assessed in twenty-seven long term meditators (average 4.21 years) both retrospectively (time one) and prospectively at one month (time two) and six months (time three) following a meditation retreat. At both time one and time three subjects reported significantly more positive effects than negative effects from meditation. However, of the twenty-seven subjects, seventeen (62.9%) reported at least one adverse effect, and two (7.4%) suffered profound adverse effects. When subjects at time one were divided into three groups based on length of practice (16.1 months; 41.1 months; 105 months) there were no significant differences in adverse effects. How the data should be interpreted, and their implications both for the clinical and psychotherapeutic use of meditation as a relaxation/self control strategy, and as a technique for facilitating personal and spiritual growth, are discussed. Limitations of the study and suggestions for future research are also offered.
INTRODUCTION
Although the clinical use of relaxation strategies have shown positive effects in arousal reduction, there is a small but growing literature pointing out some of the potential adverse effects of these strategies. For example, Lazarus and Mayne (1) (p. 261) cited such negative effects for progressive, deep muscle relaxation as "relaxation induced anxiety and panic, paradoxical increases in tension, and parasympathetic rebound." There have been similar reports of negative effects for meditation (2-5). These reports indicate that meditation may be contraindicated for those with certain types of psychiatric illness (2); that too much daily meditation may precipitate psychiatric illness and impaired reality testing (4).
Most of these case reports were with short term meditators. However, in a reanalysis of his data, Otis (5) reported that negative effects of meditation (Transcendental Meditation) were stronger in 18 month meditators than in 3-6 month meditators. Further, even teacher trainees of TM with an average of 46.7 months practice, continued to report the same adverse effects. Otis concluded his study by noting that although 52-64% of his subjects did not list a single adverse effect, that the number of those reporting adverse effects was sufficiently high to warrant further investigation.
The current study can be seen as both a replication (with a different population) and an extension of the Otis study in two ways. First, adverse effects were assessed both retrospectively (as did Otis) as well as prospectively. Secondly, the longest term meditation group in Otis's study was 46.7 months, whereas in this study the middle group is 47.1 months, and the longest group is 105 months.
METHODOLOGY
Subjects and Setting
Subjects were 27 individuals, 17 men and 10 women, with a mean age of 35.6 years (sd 13.2), who had signed up for an intensive Vipassana meditation retreat in Barre, Mass, and agreed to participate in the research study. This number who agreed to participate represented 25% of those who were attending the retreat. All subjects had meditated previously, with the average length of meditation experience 4.27 years (sd 3.32). Seventy percent meditated regularly, more than an hour a day. Two thirds had previously practiced Vipassana; and the remaining 33.3% practiced different types of concentrative or opening-up types of meditation (eg., mantra; silent; mindfulness; Soto Zen; breathing concentration; yoga; visualization). A little less than 1/4 of the group were married; over 70% had completed college; over 1/3 were atheist/agnostic; and over 50% were in professional careers.
Grouping by Length of Practice
For some of the analyses, the meditators were divided into three groupings based on length of practice. Group one (n= 10) had practiced two years or less. Test Time One average was 16.7 months practice, approximately 45 minutes a day, 80% regular meditators. Group 2 had practiced from over two years to less than seven years. Test Time One average was 47.1 months, approximately 45 minutes a day, 88.8% regular meditators. Group three (N=8) had practiced seven years or more. Test Time One average was 105 months, 75% were regular meditators, over an hour a day.
Nature of Vipassana Meditation
The meditative technique practiced at the retreat was Vipassana, part of the Theravadan Buddhist tradition. Vipassana meditation is a mindfulness type of meditation practice, a quieting technique designed to observe the mind and develop concentration. The individual is instructed to develop a "bare awareness," observing "whatever comes into awareness" without judging or evaluating (6). Individuals filling out the questionnaire had chosen either to attend a two week or three month meditation retreat. In the retreat, the day is structured into 45 minute to one and one-quarter hour segments beginning at 5:30 a.m. until 10 p.m. Formal meditation, both sitting and walking, occurs a minimum often hours per day. Further, the explicit demand characteristics of the retreat are that mindfulness meditation should be practiced at all times during the day, from when the eyes first open in the morning, to when they close at night. Silence at meals and all other times throughout the retreat is observed by the meditators except for sessions with teachers, which occur once every few days.
Method of Assessment
General effects of meditation were assessed via a paper and pencil questionnaire as part of two larger questionnaires on 1) Adherence, Expectation, Motivation; and 2) Mode of Control. The questions on Meditation Effects followed three prior questions asking 1) Why had the individual started meditation; 2) What did they perceive to be the qualities of a gifted meditator; and 3) What specifically did they hope to get from the current retreat. These questions were designed to assess "expectation effects." Subjects were then provided space to list (in an open ended format) the effects of meditation on their life under three categories 1) Positive influences 2) Adverse influences; and 3) General influences.
Data Collection and Analysis
A questionnaire was filled out before the meditators entered the retreat (retrospective-time one) and information was then gathered prospectively at one month (time two) and six months (time three) after the end of each retreat. Each individual who did not respond to the one month or six month follow-up within two weeks was sent a second form requesting compliance.
Three types of data analysis were performed: to compare responders to non-responders; to compare frequency of adverse effects to positive effects; and general descriptive statistics to examine the nature of the adverse effects. Regarding non-responders, of the 27 individuals assessed at time one, 16 (59.3%) ruled out the questionnaire at time two; and 13 (48.1 %) at time three. To assess whether there were differences in those who responded versus those who did not, a Fisher exact chi-square (7) analysis was used to compare differences between those who completed follow-up questionnaires and those who did not. Two four celled chi-square were performed. The first, comparing time one and time two, examined those who reported adverse effects and those who did not at time one in terms of those who took the assessment at time two and those who did not. The second chi-square made a similar comparison for time one and time three. There were no significant differences in either case.
To compare the frequency of adverse and positive effects, a non-parametric sign test (7) was used to compare the reporting of at least one adverse and/or positive influence. On the questionnaire an individual was free to report one or more adverse effects (or none) and/or one or more positive effects (or none). For this analysis, regardless of frequency or intensity, a person was given either a 1 or 0 depending upon whether there was at least one positive effect, and a 1 or 0 depending upon if there was at least one negative effect. The sign test was used to determine whether there were more of one type of effect than another.
RESULTS
Frequency of Adverse and Positive Effects Compared
Subjects reported significantly more positive than negative effects from meditation at time one (2 tailed p=.002); and at time three (p=.0215).
Adverse Effects
Of the twenty-seven subjects, seventeen (62.9%) reported at least one adverse effect at one of the three time periods. The frequency of adverse effects was not affected by length of practice (chi-square=3.68; df=2; p=.16). Yet the trend is in the opposite direction from what one might expect: the fewest individuals reporting adverse effects were in group one (40%), which had practiced less than two years; and the highest frequency of subjects reporting adverse effects was from group three (75%), which had practiced the longest, over 8.5 years. These results were similar both retrospectively (time one) as well as prospectively (time two, time three).
Two (7.4%) of the twenty-seven individuals suffered profound adverse effects of such intensity that they stopped meditating. Both subjects were male, but one was in group one (shortest length of practice) who had taken the two week retreat; and the other was in group three (longest length of practice) and had taken the three month retreat. The group one individual wrote at one month follow-up that the retreat left him totally disoriented: "confused, spaced out, quit meditation since retreat."
The group three individual noted at the six month follow-up:
Of those reporting adverse effects, intrapersonal were mentioned by 13 (76.4%); interpersonal by three (17.6%); and societal by three (17.6%) (More than one could be listed by an individual).
Intrapersonal adverse effects could be divided, heuristically, into four groupings. The first was increased negativity, which included statements such as increased awareness of negative qualities and emotions within myself (e.g., more judgmental, increased negative emotions, more emotional pain; increased fears and anxiety; more high strung. The second was increased disorientation, which included statements such as "confused about who I am; "loss of orientation; "loss of self'; "becoming aware of how low my self image is, how often I get down on myself;" "a feeling of incompleteness, that I need something else"; decreased attentional clarity: more spaced out, confused mind, ego strain; less motivated in life. The third was addicted to meditation, including such statements as "attached to quiet and withdrawal"; feel I am missing something between meditation retreats. And finally, boredom and pain.
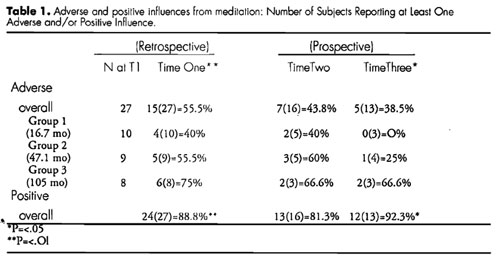
Table 1. Adverse and positive influences from meditation: Number of Subjects Reporting at Least One Adverse and/or Positive Influence.
Examples of worsened interpersonal relationships included "my family objects; I meditate as alternative to people; increased awareness of negative qualities of others, more judgmental of others, feel "false" superiority; increased discomfort with current friends; realize how bad my home situation is." Finally, examples of societal adverse effects included feelings of increased alienation from society; more uncomfortable in real world; hypersensitive to city environment; hard to adjust to the world.
Positive effects.
As noted in Table 1, eighty-eight per-cent (24 of 27) individuals listed positive effects at time one; 13 of 16 (81.3%) individuals at time two; and 12 of 13 (92.3%) at time three. These positive influences included greater happiness and joy; more positive thinking, more self-confidence; better ability to get things done (more effective); better problem solving; more accepting, compassionate, tolerant to self, and to others; more relaxed, less stressed, more resilient; better able to control feelings.
DISCUSSION
This preliminary investigation of long term meditators showed adverse effects occurring in 38% to 55.5% of the individuals reporting at different time periods. These figures, based on Vipassana meditation developed within the Buddhist tradition, is comparable to the 36% to 48% adverse effects reported in the Otis (5) study (with Transcendental Meditation developed within the Hindu/Vedic tradition). Further, rather than adverse effects decreasing based on length of practice, there is an increase in the percentage of those who report adverse effects based on the length of practice. This finding also replicates Otis's earlier finding that the adverse-effects of meditation (Transcendental Meditation) were stronger in 18 month meditators than in 3-6 month meditators, and even teacher trainees of TM with an average of 46.7 months practice, continued to report the same adverse effects. In this study, 75% of subjects with 105 months meditation experience reported adverse effects, compared to 40% of those with 16.7 months experience.
At first glance these data appear perplexing. With this high a percentage of self-reported adverse influences, why do these subjects continue to meditate, and even attend an intensive meditation retreat? Certainly one possibility is that the individuals must feel that, at some level, the positive benefits of meditation outweigh the negative. As noted, the data indicate that nearly 90% of the individuals at pretest cited positive influences of meditation; and expectation effects for the individuals regarding meditation at time one were 100% positive.
Second, individuals that listed an adverse influence often noted that there was a positive aspect to it, either currently, or within a philosophical context. One person noted; "-my family objects to my participation in the Buddhist way, but they enjoy being around me more". Another noted (time two) "brief but powerful experience of egolessness which brought deep terror and insecurity caused by reflex of mind. This is temporary; the fear will pass." At time three, this person said there were no adverse effects, noting that in meditation he is able to see that life is really "a roller coaster of powerfully pleasant and unpleasant experiences. Over time I learned the patience and forbearance and equilibrium to treat pleasant and unpleasant alike, with the same unattached awareness. This leads to a wonderful sense of strength and a lessening of fear." Thus, for some individuals, the adverse effects seem to be transformed over time, and are seen not as problems, but as something from which a person can learn.
One especially thoughtful and insightful explanation and description of this issue based on personal experience was given by another participant. His notes were quite instructive, and are therefore cited here in some detail.
As background, he noted that for two years he was disabled with active suicidal depression, including two hospitalizations and many forms of treatment, including psychotherapy, bioenergetic therapy, drug treatments of many kinds and electroconvulsive therapy. He stated that:
The above account suggest that for one individual, the adverse effects were part of positive personal transformation, but for his friend, they were not. Similarly, in this study, there were those for whom positive effects outweighed the adverse effects; but there were also two for whom the adverse effects forced the individual to stop meditating. And one individual noted that she realized that what she needed was psychological insight, not "bare awareness" of meditation.
Clinicians and health care professionals may use meditation as a relaxation technique (8) and as an adjunct in psychotherapy (9-11), and therefore should be aware of these possible adverse effects. Further, individuals may practice meditation for a variety of reasons, ranging from relaxation to personal and spiritual development (12,13). Some of these individuals may develop emotional, physical, and/or psychosomatic adverse effects, as this study indicates. Again, it is important that the clinician be sensitive to these adverse effects, the potential developmental issues, and the philosophical context in which meditation is being practiced. For example, the technique of meditation can occur within a context in which going beyond individual ego, learning surrender, and ultimate trust of the universe are positively valued. Meditation may be compelling for many individuals on different levels. Self-regulation goals can include mental peace and equanimity; and greater emotional discipline and concentration. Self-liberation goals can involve going beyond personal ego to an experiential belief about the sacred nature of the universe, a deepening of compassion; and an increased sensitivity and efforts to help end suffering in oneself and others. Depending upon the health care provider's orientation, these may or not be seen as signs of psychological well being or goals of positive health (14-17). Often a therapist may inappropriately pathologize that which does not fit neatly into his/her orientation.
On the other hand, the attainment of positive psychological and/or spiritual well being can be exceptionally difficult (16). At the risk of mixing nontheistic Buddhist and theistic Jewish metaphors, the sages of old reported in the Talmud nearly two thousand years ago the story of four Rabbis who entered Pardes to seek enlightenment. One dies, one becomes an apostate, one goes crazy; and only one returns with wisdom. These findings from this study cannot be easily dismissed, and suggest the critical importance of being sensitive to the adverse influences in short, as well as long term meditators. These potential negative effects may be true not only for meditation as relaxation, but also for meditation as a spiritual path.
PROBLEMS WITH THE STUDY AND FUTURE DIRECTIONS
Although collecting research data always presents some problems, collecting data from meditators presents special problems. For example, one commented "I found myself tense, angry, spaced out taking (the questionnaire) the second time (right after the retreat). I also found it painful and did not like doing it at all." Another noted "I am sorry to foul up your study, but I no longer feel able to make accurate generalizations about myself... one no longer knows 'what' one 'is' except in the moment -- which makes filling out this form nigh impossible."
Problems of the size of the sample, the low return rate, and the nature of questionnaire data in general, make it necessary to be cautious in generalizing from this study. Future research should attempt to determine whether it is possible to be more precisely predict, using psychological measures of defensiveness, ego strength, tolerance of ambiguity, attentional absorption, whether there is a certain subset of individuals who have more serious adverse effects. In addition, this study clearly highlights the importance of obtaining prospective, in addition to retrospective data. However, because this study so closely replicates the previous study of Otis, using a different meditation population, it does add one more piece to our understanding of adverse effects.
This article suggests a middle road, between uncritical hosannahs of meditation's effectiveness, and equally uncritical dismissal of that which does not neatly conform to the biases of rationalistic science. On the one hand, we as scientists and therapists may need to be open to exploring ultimate issues and world views which do not neatly fit within our preexisting paradigm. On the other hand, we also need to be careful that we not allow our belief systems to keep us from blindly seeing growth where there may in fact be harm occurring.
_______________
REFERENCES
1. Lazarus, AA. and Mayne, TM Relaxation: Some limitations, side effects, and proposed solutions. Psychotherapy 27,2,261266, (1990).
2. Walsh, R. and Rauche, L. The precipitation of acute psychoses by intensive meditation in individuals with a history of schizophrenia. American Journal of Psychiatry 138(8), 185-186, (1979).
3. Lazarus, AA (Psychiatric problems precipitated by transcendental meditation. Psychological Reports 10,39-74, 1975).
4. French, AP, Smid, AC, and Ingalls, E. Transcendental meditation, altered reality testing and behavioral change: A case report. Journal of Nervous and Mental Disease 161, 55-58, (1975).
5. Otis, LS. Adverse effects of transcendental meditation. In DH Shapiro and RN Walsh (Eds). Meditation: Classic and Contemporary Perspectives. New York: Aldine. 201-208, (1984).
6. Goldstein, J. The experience of insight, Santa Cruz, Ca: Unity Press, (1976).
7. Siegel, S.. Nonparametric statistics for the behavioral sciences. New York: McGraw Hill, (1956)
8. Benson, H., The Relaxation Response New York: Morrow, (1975).
9. Shapiro, DH and Giber, D Z Medication and psychotherapeutic effects. Archives of General Psychiatry, 35,294-302,.(1978).
10. Kutz, I; Borysenko, JZ, and Benson, H Meditation and Psychotherapy. American Journal of Psychiatry 142:1,1-8, (1985).
11. Shapiro, D. H. Comparison of meditation with other self-control strategies: biofeedback, hypnosis, progressive relaxation: A review of the clinical and physiological literature. American Journal of Psychiatry, 139(3),267-274, 1982.
12. Shapiro, D. H. Meditation: Self Regulation Strategy and Altered States of Consciousness, New York: Aldine, (1980).
13. Shapiro, D.H. and Walsh, R.N, (Eds,) Meditation: Classic and Contemporary Perspectives. New York: Aldine, (1984)
14. Shapiro, DH. Meditation, self-control, and control by a benevolent other: Issues of content and context. In Psychotherapy, Medication, and Health M. Kwee (Ed,) London: East-West, pp. 65-123, (1990).
15. Walsh, RN., The consciousness disciplines and the behavioral sciences. American Journal of Psychiatry, 137, (6), 663-673, (1980).
16. Walsh, RN and D. H. Shapiro (Eds) Beyond Health and Normality. Toward a vision of exceptional Psychological health New York: Van Nostrand Reinhold, 371-387.
17. Grof, S; and Grof, C. (Eds) Spiritual Emergencies: When Personal Transformation becomes a crisis. Los Angeles: Tarcher, (1989).
18. Shapiro, DH. The Role of Control and Self-Control in Psychotherapy and Health Care. New York: John Wiley, (in press).
19. Shapiro, DH. The Human Quest for Control. Los Angeles: Tarcher, (in press).
20. Shapiro, DH. The Shapiro Control Inventory (SCl): Measuring Personal, Interpersonal and Spiritual Sense of Control. Palo Alto: Behaviordyne, (1992).
Index Terms
Negative effects, Vipassana meditation, relaxation
Requests for Reprints:
Deane H. Shapiro, Jr., Ph.D.
1009 Canyon View Drive
Laguna Beach, CA 92651
Deane H. Shapiro, Jr., Ph.D. is an Associate Professor in Residence, Department of Psychiatry and Human Behavior, California College of Medicine, University of California, Irvine. Portions of this article have been presented at the International Association for Applied Psychology (Kyoto, Japan, 1990); First International Conference on Psychotherapy, Meditation, and Health (Amsterdam, Holland, 1990); and the Institute of Noetic Sciences Third Annual Meditation Research Seminar (Esalen, Big Sur, California, 1991).
by Deane H. Shapiro, Jr., Ph.D.
International Journal of Psychosomatics, Vol. 39 (Nos. 1-4), 1992 63
Manuscript submitted June 30, 1991 and accepted May 1 1992.
NOTICE: THIS WORK MAY BE PROTECTED BY COPYRIGHT
YOU ARE REQUIRED TO READ THE COPYRIGHT NOTICE AT THIS LINK BEFORE YOU READ THE FOLLOWING WORK, THAT IS AVAILABLE SOLELY FOR PRIVATE STUDY, SCHOLARSHIP OR RESEARCH PURSUANT TO 17 U.S.C. SECTION 107 AND 108. IN THE EVENT THAT THE LIBRARY DETERMINES THAT UNLAWFUL COPYING OF THIS WORK HAS OCCURRED, THE LIBRARY HAS THE RIGHT TO BLOCK THE I.P. ADDRESS AT WHICH THE UNLAWFUL COPYING APPEARED TO HAVE OCCURRED. THANK YOU FOR RESPECTING THE RIGHTS OF COPYRIGHT OWNERS.
Adverse effects of meditation were assessed in twenty-seven long term meditators (average 4.21 years) both retrospectively (time one) and prospectively at one month (time two) and six months (time three) following a meditation retreat. At both time one and time three subjects reported significantly more positive effects than negative effects from meditation. However, of the twenty-seven subjects, seventeen (62.9%) reported at least one adverse effect, and two (7.4%) suffered profound adverse effects. When subjects at time one were divided into three groups based on length of practice (16.1 months; 41.1 months; 105 months) there were no significant differences in adverse effects. How the data should be interpreted, and their implications both for the clinical and psychotherapeutic use of meditation as a relaxation/self control strategy, and as a technique for facilitating personal and spiritual growth, are discussed. Limitations of the study and suggestions for future research are also offered.
INTRODUCTION
Although the clinical use of relaxation strategies have shown positive effects in arousal reduction, there is a small but growing literature pointing out some of the potential adverse effects of these strategies. For example, Lazarus and Mayne (1) (p. 261) cited such negative effects for progressive, deep muscle relaxation as "relaxation induced anxiety and panic, paradoxical increases in tension, and parasympathetic rebound." There have been similar reports of negative effects for meditation (2-5). These reports indicate that meditation may be contraindicated for those with certain types of psychiatric illness (2); that too much daily meditation may precipitate psychiatric illness and impaired reality testing (4).
Most of these case reports were with short term meditators. However, in a reanalysis of his data, Otis (5) reported that negative effects of meditation (Transcendental Meditation) were stronger in 18 month meditators than in 3-6 month meditators. Further, even teacher trainees of TM with an average of 46.7 months practice, continued to report the same adverse effects. Otis concluded his study by noting that although 52-64% of his subjects did not list a single adverse effect, that the number of those reporting adverse effects was sufficiently high to warrant further investigation.
The current study can be seen as both a replication (with a different population) and an extension of the Otis study in two ways. First, adverse effects were assessed both retrospectively (as did Otis) as well as prospectively. Secondly, the longest term meditation group in Otis's study was 46.7 months, whereas in this study the middle group is 47.1 months, and the longest group is 105 months.
METHODOLOGY
Subjects and Setting
Subjects were 27 individuals, 17 men and 10 women, with a mean age of 35.6 years (sd 13.2), who had signed up for an intensive Vipassana meditation retreat in Barre, Mass, and agreed to participate in the research study. This number who agreed to participate represented 25% of those who were attending the retreat. All subjects had meditated previously, with the average length of meditation experience 4.27 years (sd 3.32). Seventy percent meditated regularly, more than an hour a day. Two thirds had previously practiced Vipassana; and the remaining 33.3% practiced different types of concentrative or opening-up types of meditation (eg., mantra; silent; mindfulness; Soto Zen; breathing concentration; yoga; visualization). A little less than 1/4 of the group were married; over 70% had completed college; over 1/3 were atheist/agnostic; and over 50% were in professional careers.
Grouping by Length of Practice
For some of the analyses, the meditators were divided into three groupings based on length of practice. Group one (n= 10) had practiced two years or less. Test Time One average was 16.7 months practice, approximately 45 minutes a day, 80% regular meditators. Group 2 had practiced from over two years to less than seven years. Test Time One average was 47.1 months, approximately 45 minutes a day, 88.8% regular meditators. Group three (N=8) had practiced seven years or more. Test Time One average was 105 months, 75% were regular meditators, over an hour a day.
Nature of Vipassana Meditation
The meditative technique practiced at the retreat was Vipassana, part of the Theravadan Buddhist tradition. Vipassana meditation is a mindfulness type of meditation practice, a quieting technique designed to observe the mind and develop concentration. The individual is instructed to develop a "bare awareness," observing "whatever comes into awareness" without judging or evaluating (6). Individuals filling out the questionnaire had chosen either to attend a two week or three month meditation retreat. In the retreat, the day is structured into 45 minute to one and one-quarter hour segments beginning at 5:30 a.m. until 10 p.m. Formal meditation, both sitting and walking, occurs a minimum often hours per day. Further, the explicit demand characteristics of the retreat are that mindfulness meditation should be practiced at all times during the day, from when the eyes first open in the morning, to when they close at night. Silence at meals and all other times throughout the retreat is observed by the meditators except for sessions with teachers, which occur once every few days.
Method of Assessment
General effects of meditation were assessed via a paper and pencil questionnaire as part of two larger questionnaires on 1) Adherence, Expectation, Motivation; and 2) Mode of Control. The questions on Meditation Effects followed three prior questions asking 1) Why had the individual started meditation; 2) What did they perceive to be the qualities of a gifted meditator; and 3) What specifically did they hope to get from the current retreat. These questions were designed to assess "expectation effects." Subjects were then provided space to list (in an open ended format) the effects of meditation on their life under three categories 1) Positive influences 2) Adverse influences; and 3) General influences.
Data Collection and Analysis
A questionnaire was filled out before the meditators entered the retreat (retrospective-time one) and information was then gathered prospectively at one month (time two) and six months (time three) after the end of each retreat. Each individual who did not respond to the one month or six month follow-up within two weeks was sent a second form requesting compliance.
Three types of data analysis were performed: to compare responders to non-responders; to compare frequency of adverse effects to positive effects; and general descriptive statistics to examine the nature of the adverse effects. Regarding non-responders, of the 27 individuals assessed at time one, 16 (59.3%) ruled out the questionnaire at time two; and 13 (48.1 %) at time three. To assess whether there were differences in those who responded versus those who did not, a Fisher exact chi-square (7) analysis was used to compare differences between those who completed follow-up questionnaires and those who did not. Two four celled chi-square were performed. The first, comparing time one and time two, examined those who reported adverse effects and those who did not at time one in terms of those who took the assessment at time two and those who did not. The second chi-square made a similar comparison for time one and time three. There were no significant differences in either case.
To compare the frequency of adverse and positive effects, a non-parametric sign test (7) was used to compare the reporting of at least one adverse and/or positive influence. On the questionnaire an individual was free to report one or more adverse effects (or none) and/or one or more positive effects (or none). For this analysis, regardless of frequency or intensity, a person was given either a 1 or 0 depending upon whether there was at least one positive effect, and a 1 or 0 depending upon if there was at least one negative effect. The sign test was used to determine whether there were more of one type of effect than another.
RESULTS
Frequency of Adverse and Positive Effects Compared
Subjects reported significantly more positive than negative effects from meditation at time one (2 tailed p=.002); and at time three (p=.0215).
Adverse Effects
Of the twenty-seven subjects, seventeen (62.9%) reported at least one adverse effect at one of the three time periods. The frequency of adverse effects was not affected by length of practice (chi-square=3.68; df=2; p=.16). Yet the trend is in the opposite direction from what one might expect: the fewest individuals reporting adverse effects were in group one (40%), which had practiced less than two years; and the highest frequency of subjects reporting adverse effects was from group three (75%), which had practiced the longest, over 8.5 years. These results were similar both retrospectively (time one) as well as prospectively (time two, time three).
Two (7.4%) of the twenty-seven individuals suffered profound adverse effects of such intensity that they stopped meditating. Both subjects were male, but one was in group one (shortest length of practice) who had taken the two week retreat; and the other was in group three (longest length of practice) and had taken the three month retreat. The group one individual wrote at one month follow-up that the retreat left him totally disoriented: "confused, spaced out, quit meditation since retreat."
The group three individual noted at the six month follow-up:
My experience of returning from the retreat was a difficult one. The mind set values that the retreat cultivated felt out of synch with the world I came back to and I've been slowly digesting the transformative changes that the retreat generated. Lots of depression, confusion, struggle during the last six months....experienced some severe shaking and energy releasing; eventually injured my back and stopped doing Vipassana practice.
Of those reporting adverse effects, intrapersonal were mentioned by 13 (76.4%); interpersonal by three (17.6%); and societal by three (17.6%) (More than one could be listed by an individual).
Intrapersonal adverse effects could be divided, heuristically, into four groupings. The first was increased negativity, which included statements such as increased awareness of negative qualities and emotions within myself (e.g., more judgmental, increased negative emotions, more emotional pain; increased fears and anxiety; more high strung. The second was increased disorientation, which included statements such as "confused about who I am; "loss of orientation; "loss of self'; "becoming aware of how low my self image is, how often I get down on myself;" "a feeling of incompleteness, that I need something else"; decreased attentional clarity: more spaced out, confused mind, ego strain; less motivated in life. The third was addicted to meditation, including such statements as "attached to quiet and withdrawal"; feel I am missing something between meditation retreats. And finally, boredom and pain.
Table 1. Adverse and positive influences from meditation: Number of Subjects Reporting at Least One Adverse and/or Positive Influence.
Examples of worsened interpersonal relationships included "my family objects; I meditate as alternative to people; increased awareness of negative qualities of others, more judgmental of others, feel "false" superiority; increased discomfort with current friends; realize how bad my home situation is." Finally, examples of societal adverse effects included feelings of increased alienation from society; more uncomfortable in real world; hypersensitive to city environment; hard to adjust to the world.
Positive effects.
As noted in Table 1, eighty-eight per-cent (24 of 27) individuals listed positive effects at time one; 13 of 16 (81.3%) individuals at time two; and 12 of 13 (92.3%) at time three. These positive influences included greater happiness and joy; more positive thinking, more self-confidence; better ability to get things done (more effective); better problem solving; more accepting, compassionate, tolerant to self, and to others; more relaxed, less stressed, more resilient; better able to control feelings.
DISCUSSION
This preliminary investigation of long term meditators showed adverse effects occurring in 38% to 55.5% of the individuals reporting at different time periods. These figures, based on Vipassana meditation developed within the Buddhist tradition, is comparable to the 36% to 48% adverse effects reported in the Otis (5) study (with Transcendental Meditation developed within the Hindu/Vedic tradition). Further, rather than adverse effects decreasing based on length of practice, there is an increase in the percentage of those who report adverse effects based on the length of practice. This finding also replicates Otis's earlier finding that the adverse-effects of meditation (Transcendental Meditation) were stronger in 18 month meditators than in 3-6 month meditators, and even teacher trainees of TM with an average of 46.7 months practice, continued to report the same adverse effects. In this study, 75% of subjects with 105 months meditation experience reported adverse effects, compared to 40% of those with 16.7 months experience.
At first glance these data appear perplexing. With this high a percentage of self-reported adverse influences, why do these subjects continue to meditate, and even attend an intensive meditation retreat? Certainly one possibility is that the individuals must feel that, at some level, the positive benefits of meditation outweigh the negative. As noted, the data indicate that nearly 90% of the individuals at pretest cited positive influences of meditation; and expectation effects for the individuals regarding meditation at time one were 100% positive.
Second, individuals that listed an adverse influence often noted that there was a positive aspect to it, either currently, or within a philosophical context. One person noted; "-my family objects to my participation in the Buddhist way, but they enjoy being around me more". Another noted (time two) "brief but powerful experience of egolessness which brought deep terror and insecurity caused by reflex of mind. This is temporary; the fear will pass." At time three, this person said there were no adverse effects, noting that in meditation he is able to see that life is really "a roller coaster of powerfully pleasant and unpleasant experiences. Over time I learned the patience and forbearance and equilibrium to treat pleasant and unpleasant alike, with the same unattached awareness. This leads to a wonderful sense of strength and a lessening of fear." Thus, for some individuals, the adverse effects seem to be transformed over time, and are seen not as problems, but as something from which a person can learn.
One especially thoughtful and insightful explanation and description of this issue based on personal experience was given by another participant. His notes were quite instructive, and are therefore cited here in some detail.
As background, he noted that for two years he was disabled with active suicidal depression, including two hospitalizations and many forms of treatment, including psychotherapy, bioenergetic therapy, drug treatments of many kinds and electroconvulsive therapy. He stated that:
For me meditation is by far the most effective form of therapy... it is not a palliative; rather it eliminates the cause of mental suffering at its very roots. However, I have found in my own experience that I needed a certain degree of mental health and stability before I could undertake intensive meditation. Most psychotherapy seems to me a way of strengthening the ego. Meditation is a way of tearing it down.
The paradox is that one seems to need a relatively strong ego in order to endure its removal... Three months of intensive uninterrupted meditation seemed to me very much like a controlled breakdown, paralleling in many marked ways my own breakdown four years ago.
In order to reach a deeper stability, one becomes fundamentally destabilized. To undergo this, one needs considerable preliminary strength and faith. If that strength and faith do not exist, intensive meditation can be dangerous. One of my colleagues during the three month retreat was asked to leave early because he was becoming seriously unstable and delusive. Degeneration continued at home for a month and a half. Eventually he attempted suicide because he had "failed" to become enlightened. He is now hospitalized and is seriously mentally ill.
The above account suggest that for one individual, the adverse effects were part of positive personal transformation, but for his friend, they were not. Similarly, in this study, there were those for whom positive effects outweighed the adverse effects; but there were also two for whom the adverse effects forced the individual to stop meditating. And one individual noted that she realized that what she needed was psychological insight, not "bare awareness" of meditation.
Clinicians and health care professionals may use meditation as a relaxation technique (8) and as an adjunct in psychotherapy (9-11), and therefore should be aware of these possible adverse effects. Further, individuals may practice meditation for a variety of reasons, ranging from relaxation to personal and spiritual development (12,13). Some of these individuals may develop emotional, physical, and/or psychosomatic adverse effects, as this study indicates. Again, it is important that the clinician be sensitive to these adverse effects, the potential developmental issues, and the philosophical context in which meditation is being practiced. For example, the technique of meditation can occur within a context in which going beyond individual ego, learning surrender, and ultimate trust of the universe are positively valued. Meditation may be compelling for many individuals on different levels. Self-regulation goals can include mental peace and equanimity; and greater emotional discipline and concentration. Self-liberation goals can involve going beyond personal ego to an experiential belief about the sacred nature of the universe, a deepening of compassion; and an increased sensitivity and efforts to help end suffering in oneself and others. Depending upon the health care provider's orientation, these may or not be seen as signs of psychological well being or goals of positive health (14-17). Often a therapist may inappropriately pathologize that which does not fit neatly into his/her orientation.
On the other hand, the attainment of positive psychological and/or spiritual well being can be exceptionally difficult (16). At the risk of mixing nontheistic Buddhist and theistic Jewish metaphors, the sages of old reported in the Talmud nearly two thousand years ago the story of four Rabbis who entered Pardes to seek enlightenment. One dies, one becomes an apostate, one goes crazy; and only one returns with wisdom. These findings from this study cannot be easily dismissed, and suggest the critical importance of being sensitive to the adverse influences in short, as well as long term meditators. These potential negative effects may be true not only for meditation as relaxation, but also for meditation as a spiritual path.
PROBLEMS WITH THE STUDY AND FUTURE DIRECTIONS
Although collecting research data always presents some problems, collecting data from meditators presents special problems. For example, one commented "I found myself tense, angry, spaced out taking (the questionnaire) the second time (right after the retreat). I also found it painful and did not like doing it at all." Another noted "I am sorry to foul up your study, but I no longer feel able to make accurate generalizations about myself... one no longer knows 'what' one 'is' except in the moment -- which makes filling out this form nigh impossible."
Problems of the size of the sample, the low return rate, and the nature of questionnaire data in general, make it necessary to be cautious in generalizing from this study. Future research should attempt to determine whether it is possible to be more precisely predict, using psychological measures of defensiveness, ego strength, tolerance of ambiguity, attentional absorption, whether there is a certain subset of individuals who have more serious adverse effects. In addition, this study clearly highlights the importance of obtaining prospective, in addition to retrospective data. However, because this study so closely replicates the previous study of Otis, using a different meditation population, it does add one more piece to our understanding of adverse effects.
This article suggests a middle road, between uncritical hosannahs of meditation's effectiveness, and equally uncritical dismissal of that which does not neatly conform to the biases of rationalistic science. On the one hand, we as scientists and therapists may need to be open to exploring ultimate issues and world views which do not neatly fit within our preexisting paradigm. On the other hand, we also need to be careful that we not allow our belief systems to keep us from blindly seeing growth where there may in fact be harm occurring.
_______________
REFERENCES
1. Lazarus, AA. and Mayne, TM Relaxation: Some limitations, side effects, and proposed solutions. Psychotherapy 27,2,261266, (1990).
2. Walsh, R. and Rauche, L. The precipitation of acute psychoses by intensive meditation in individuals with a history of schizophrenia. American Journal of Psychiatry 138(8), 185-186, (1979).
3. Lazarus, AA (Psychiatric problems precipitated by transcendental meditation. Psychological Reports 10,39-74, 1975).
4. French, AP, Smid, AC, and Ingalls, E. Transcendental meditation, altered reality testing and behavioral change: A case report. Journal of Nervous and Mental Disease 161, 55-58, (1975).
5. Otis, LS. Adverse effects of transcendental meditation. In DH Shapiro and RN Walsh (Eds). Meditation: Classic and Contemporary Perspectives. New York: Aldine. 201-208, (1984).
6. Goldstein, J. The experience of insight, Santa Cruz, Ca: Unity Press, (1976).
7. Siegel, S.. Nonparametric statistics for the behavioral sciences. New York: McGraw Hill, (1956)
8. Benson, H., The Relaxation Response New York: Morrow, (1975).
9. Shapiro, DH and Giber, D Z Medication and psychotherapeutic effects. Archives of General Psychiatry, 35,294-302,.(1978).
10. Kutz, I; Borysenko, JZ, and Benson, H Meditation and Psychotherapy. American Journal of Psychiatry 142:1,1-8, (1985).
11. Shapiro, D. H. Comparison of meditation with other self-control strategies: biofeedback, hypnosis, progressive relaxation: A review of the clinical and physiological literature. American Journal of Psychiatry, 139(3),267-274, 1982.
12. Shapiro, D. H. Meditation: Self Regulation Strategy and Altered States of Consciousness, New York: Aldine, (1980).
13. Shapiro, D.H. and Walsh, R.N, (Eds,) Meditation: Classic and Contemporary Perspectives. New York: Aldine, (1984)
14. Shapiro, DH. Meditation, self-control, and control by a benevolent other: Issues of content and context. In Psychotherapy, Medication, and Health M. Kwee (Ed,) London: East-West, pp. 65-123, (1990).
15. Walsh, RN., The consciousness disciplines and the behavioral sciences. American Journal of Psychiatry, 137, (6), 663-673, (1980).
16. Walsh, RN and D. H. Shapiro (Eds) Beyond Health and Normality. Toward a vision of exceptional Psychological health New York: Van Nostrand Reinhold, 371-387.
17. Grof, S; and Grof, C. (Eds) Spiritual Emergencies: When Personal Transformation becomes a crisis. Los Angeles: Tarcher, (1989).
18. Shapiro, DH. The Role of Control and Self-Control in Psychotherapy and Health Care. New York: John Wiley, (in press).
19. Shapiro, DH. The Human Quest for Control. Los Angeles: Tarcher, (in press).
20. Shapiro, DH. The Shapiro Control Inventory (SCl): Measuring Personal, Interpersonal and Spiritual Sense of Control. Palo Alto: Behaviordyne, (1992).
Index Terms
Negative effects, Vipassana meditation, relaxation
Requests for Reprints:
Deane H. Shapiro, Jr., Ph.D.
1009 Canyon View Drive
Laguna Beach, CA 92651
Deane H. Shapiro, Jr., Ph.D. is an Associate Professor in Residence, Department of Psychiatry and Human Behavior, California College of Medicine, University of California, Irvine. Portions of this article have been presented at the International Association for Applied Psychology (Kyoto, Japan, 1990); First International Conference on Psychotherapy, Meditation, and Health (Amsterdam, Holland, 1990); and the Institute of Noetic Sciences Third Annual Meditation Research Seminar (Esalen, Big Sur, California, 1991).